400-029-0925
400-029-0925
脑膜瘤为颅内常见良性肿瘤,生长缓慢,多表现为慢性头痛,一般无不同症状,多在中老年以后被检查发现,女性发病率高于男性。有观点认为,此病发生可能与刺激素有关,个别报道脑外伤后此病发生率也会增高。
脑膜瘤,多发生和起源于在硬脑膜上,好发于静脉窦旁、大脑镰、蝶骨脊、桥小脑角、小脑幕、鞍结节、嗅沟,海绵窦区,少数在大脑或小脑的凸面,以及脑室内。
以下是INC国际神经外科医生集团、国际神经内镜联合会执行委员会主席Henry W. S. Schroeder教授关于16个嗅沟脑膜瘤的病例解析论文交流:16 Olfactory Groove Meningiomas(16个嗅沟脑膜瘤病例)
论文英文摘要:Olfactory groove meningiomas arise from the dura around the cribriform plate and can span the anterior skull base from the crista galli to the tuberculum sella, often involving the optic pathway and anterior circulation. While there are a variety of open surgical approaches to these lesions, it is important to select the optimal approach to provide adequate exposure of the tumor and involved dura, bone, and vasculature, as well as to allow for reconstruction and closure. Postoperative complications, including cerebral edema and cerebrospinal fluid leak, may be prevented by carefully selecting and planning an appropriate surgical approach for a given lesion. In 16.2, we review the merits and drawbacks of open transcranial approaches for olfactory groove meningiomas and discuss our recommended surgical approaches and management considerations. In 16.3, we demonstrate that the supraorbital eyebrow keyhole approach allows gross total resection of small- and medium-sized olfactory groove meningiomas. The cosmetic result is usually excellent. The complications rate is low. Because of the low height of the craniotomy, visualization of the olfactory groove requires frequently endoscope assistance especially when the olfactory groove is very steep. The rate of CSF leakage and loss of olfaction is lower than with the endonasal approach. Therefore, we consider the supraorbital eyebrow approach as the procedure of choice for most olfactory groove meningiomas. In 16.4, we demonstrate that olfactory groove meningiomas are lesions of the frontal skull base that also can be approached via a transcranial route from above or an endoscopic transnasal route from below. There are three main parts of transnasal endoscopic skull base approaches for olfactory groove meningiomas: the transethmoidal, transcribriform, and transplanum. The approach can be optimally tailored to the tumor size and surgical situation, with the opening as large as necessary but as minimally invasive as possible. There are special considerations concerning patient selection and surgical technique to make an appropriate decision about the optimal approach. A successful result will owe a great deal to careful patient selection, detailed planning, and a dedicated surgical team.

中文:嗅沟脑膜瘤产生于筛板而会跨越整个颅前窝,经常会伸到视路和前循环。针对这种病变有许多开放性的手术入路,所以,重要的是选择更佳的入路,以充分暴露肿瘤、硬脑膜和血管,并允许重建和缝合。术后并发症,包括脑水肿和脑脊液泄露,可以通过仔细选择和计划适当的手术入路避免。在16.2章,我们回顾对溴沟脑膜瘤开放性经颅入路,并讨论更佳的手术入路和管理考虑。在16.3章,我们展示以眶上眉锁孔入路可以实行小中等大小嗅沟脑膜瘤的完全切除。美容效果一般很。并发症发生率很低。由于开路位置很低,为了暴露嗅沟,经常需用神经内镜辅助,在嗅沟很深的情况下。脑脊液泄露率和嗅觉功能的失去少于经鼻入路。因此,我们认为大多数情况下,对于溴沟脑膜瘤而言,眶上眉锁孔入路是更佳的入路选择。在16.4章,我们展示,溴沟脑膜瘤属于前颅底的病变,其可以通过从上方的经颅途径或者从下方的经鼻内镜途径接近。接近溴沟脑膜瘤的经鼻内镜颅底入路主要有三部分:经筛骨、经筛板和经蝶骨平台。入路可以根据肿瘤大小和手术条件进行更佳调整,切口会尽可能大,但侵入性尽可能小。对病人的选择和手术技巧有不同的考虑,以便对更佳手术入路作出适当的决定。一个成功的结果将在很大水平上归功于仔细的病人选择、详细的计划和一个专门的外科团队。
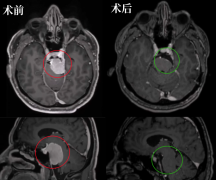
如果脑膜瘤的位置比较好,手术难度相对来说比较简单,风险比较低,容易取得较高的切除率和预后,但是手术较好能够将病灶的根部包括脑膜完整切除,这样不容易复发。如果脑膜瘤在较深的位置,例如枕骨大孔区,斜坡脑膜瘤、大脑镰脑膜瘤,那么手术难度就会较大,不容易确定较高的切除率,也不容易确定手术的顺利。脑膜瘤的手术,每多切那么一点点,复发的概率就低很多。所以,全国际的神经外科医院、神经外科医生都倾尽在顺利和神经顺利的前提下尝试更高的切除率。Henry W.S. Schroeder教授就是国际神经外科范围内少有的能做到完全切除包括嗅沟脑膜瘤在内的各种位置脑膜瘤的专家。
作为德国乃至国际神经内镜专家,Henry W.S. Schroeder教授此前曾任国际神经外科联合会(WFNS)内镜委员会主席。Henry W.S. Schroeder教授拥有20余年神经外科疾病咨询经验,其擅长领域涵盖内镜神经外科(脑积水、囊肿、脑室内病变)、内镜颅底手术(脑膜瘤、前庭神经鞘瘤、表皮样囊肿)、鼻内镜颅底手术(垂体瘤、颅咽管瘤)、周围神经手术等,经其神经内镜手术治疗的脑膜瘤、垂体瘤 、颅咽管瘤病例切除率高、治愈率高、复发率较低。

此外,Henry W.S. Schroeder教授对于国际神经外科学术研究及发展贡献卓著,他曾在各类神经外科杂志、期刊上发表了上百余篇学术论文,且与德国其他神经外科专家一起合著、编纂了《神经内镜手术》和《神经外科实用手册》等丛书,对于神经外科医生具有较大的临床实践指导意义。以其超群的神经内镜技术和深厚的学术功底,Henry W.S. Schroeder教授经常作为特邀讲师来华指导国内神经外科专家进行垂体瘤、脑膜瘤、颅咽管瘤等神经内镜手术技术培训,并多次受邀参与范围内研讨神经外科肿瘤疾病诊治的学术盛会。
相关经典案例
- 文章标题:INC德国Schroeder教授解析16个嗅沟脑膜瘤病例的完整切除手术
- 更新时间:2019-10-09 17:53:32